
The Indispensable Role of CBCT in Pre-Surgical Implant Planning
Overcoming 2D Limitations: Why 3D Vision is Crucial
When it comes to dental implant planning, seeing the complete picture makes all the difference. Traditional 2D radiography, such as Orthopantomograms (OPGs), has long been the standard tool in dentistry. However, these flat images fail to capture the true complexity of oral anatomy, often leaving dentists partially blind to critical structures.
The limitations of 2D imaging are stark. These traditional radiographs compress three-dimensional structures into a single plane, causing overlapping images that obscure vital details. This flattening effect can hide important anatomical variations or pathologies that might affect implant success. Recent clinical research highlights a concerning reality: surgeons using only OPG imaging had to unexpectedly abort 7% of implant surgeries after beginning the procedure. The reason? They discovered insufficient bone quantity or couldn't achieve primary stability – issues that remained hidden on 2D scans but would have been obvious with 3D imaging.
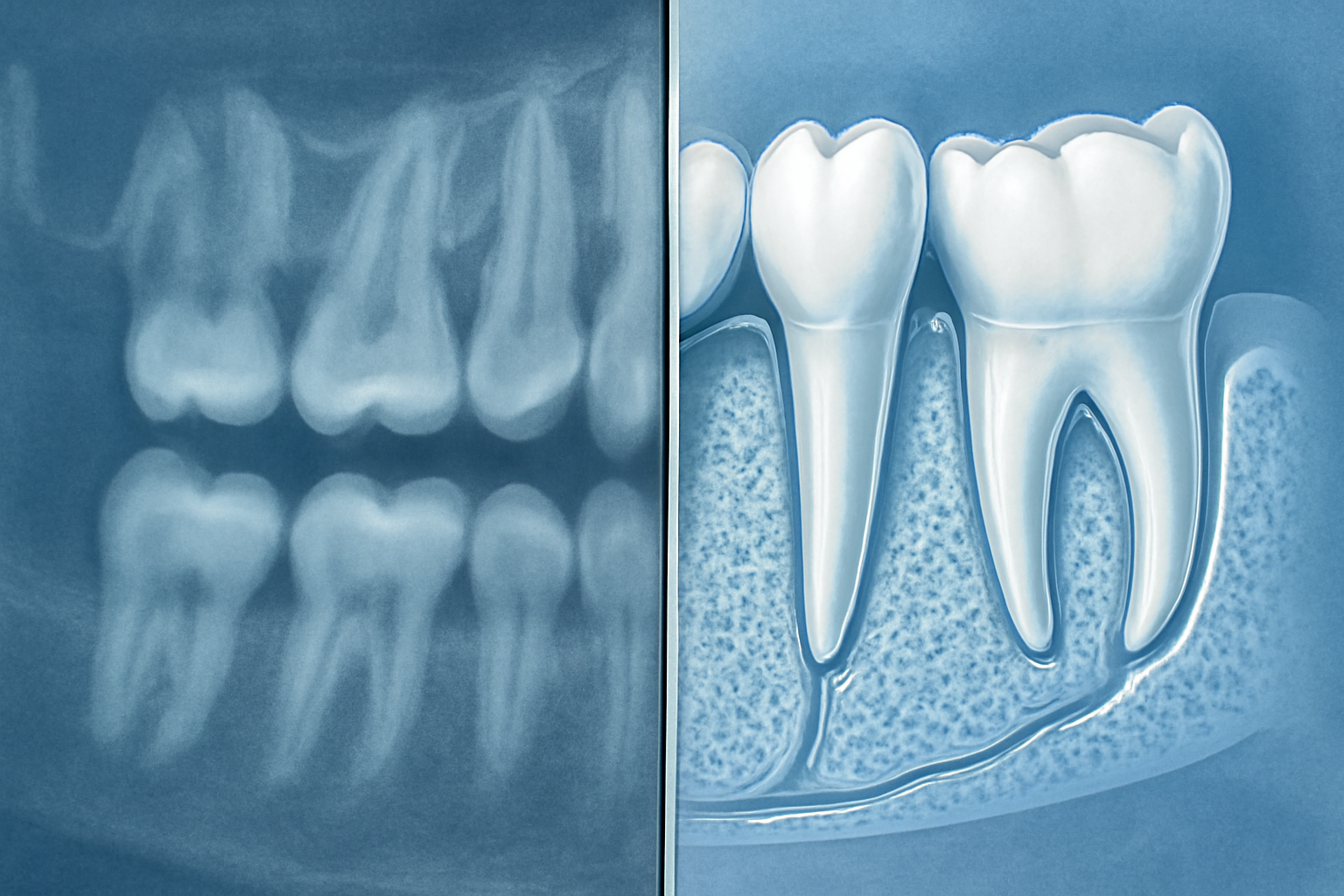
Cone Beam Computed Tomography (CBCT) addresses these shortcomings by providing comprehensive volumetric data. Unlike traditional radiography, CBCT captures the entire region of interest in three dimensions, allowing dentists to examine potential implant sites from every angle. This third dimension transforms implant planning from educated guesswork into precise surgical mapping.
The ability to view oral structures in axial, coronal, and sagittal planes gives dentists unprecedented insight into the patient's anatomy. This multi-dimensional perspective reveals the exact height, width, and depth of available bone – measurements that significantly impact implant success rates. Additionally, CBCT enables accurate evaluation of bone density, helping clinicians select appropriate implant designs and surgical protocols based on bone quality.
Precision Planning: Identifying Vital Structures and Bone Characteristics
CBCT imaging excels at revealing critical anatomical boundaries essential for safe implant placement. The technology clearly visualizes vital structures like the inferior alveolar nerve, mental foramen, maxillary sinus floor, and adjacent tooth roots – structures that might be partially or completely obscured in 2D imaging.
This precision is particularly valuable in preventing neurovascular complications, which can lead to permanent sensory disturbances, excessive bleeding, or implant failure.
 Comprehensive studies show that CBCT allows dentists to measure exact distances to these critical structures, establishing safe margins for implant placement.
Comprehensive studies show that CBCT allows dentists to measure exact distances to these critical structures, establishing safe margins for implant placement.
Beyond safety considerations, CBCT provides detailed insight into bone morphology. The technology reveals ridge contours, undercuts, concavities, and defects that might otherwise go undetected. This is especially crucial in aesthetically challenging cases or when working with compromised bone volume.
For patients with borderline bone availability, CBCT helps clinicians determine whether standard implant placement is possible or if advanced techniques like bone grafting or distraction osteogenesis are needed. The technology's ability to accurately assess bone dimensions enables precise selection of implant size, position, and angulation – all without the issues of superimposition that plague 2D imaging.
Virtual Planning and Guided Surgery: Enhancing Predictability
CBCT's full potential is realized when combined with specialized 3D planning software. This powerful combination allows dentists to perform virtual implant placement before touching the patient.
Beyond Placement: CBCT in Post-Surgical Evaluation and Future Directions
Post-Surgical Assessment and Complication Management
While the pre-surgical planning phase receives most of the attention, CBCT's value extends well beyond implant placement. In the post-surgical phase, this technology becomes an invaluable tool for monitoring healing and addressing complications.
CBCT provides detailed visualization of bone graft integration, allowing clinicians to assess the success of grafting procedures with unprecedented clarity. This 3D perspective reveals how new bone forms around the implant, which is crucial for determining long-term stability and function.
When complications arise, CBCT proves especially valuable. In fact, research shows that 22% of post-surgical CBCT scans are specifically ordered to investigate complications. This is particularly true for neurovascular trauma cases, where damage to nerves or blood vessels can cause serious patient discomfort or functional issues.
Nerve injuries, one of the most serious complications in implant dentistry, are often linked to inadequate pre-operative radiological assessment. CBCT helps both prevent these injuries and manage them when they occur by clearly showing the relationship between the implant and neural structures.
When implant retrieval becomes necessary due to failure or complications, CBCT guides the removal process by visualizing the exact position and angulation of the implant in relation to surrounding structures. This minimizes additional trauma during the retrieval process.
Though 2D intraoral radiographs remain the standard for routine post-surgical monitoring, they simply can't match CBCT's ability to reveal the full picture of peri-implant tissues in complex cases. For patients experiencing severe peri-implantitis with significant bone loss, CBCT provides critical volumetric information that guides treatment decisions.
Challenges and Limitations of CBCT in Implantology
Despite its advantages, CBCT has notable limitations.
 Metal artifacts represent one of the most significant challenges, creating bright streaks or dark areas that obscure critical details. These artifacts are particularly problematic when trying to assess bone immediately surrounding an implant, which is precisely where evaluation is most needed.
Metal artifacts represent one of the most significant challenges, creating bright streaks or dark areas that obscure critical details. These artifacts are particularly problematic when trying to assess bone immediately surrounding an implant, which is precisely where evaluation is most needed.
Another significant drawback is CBCT's poor soft tissue differentiation. Unlike medical CT or MRI, CBCT cannot clearly distinguish between various soft tissue types, limiting its usefulness for comprehensive treatment planning that involves both hard and soft tissues.
Bone density assessment, critical for implant success, remains problematic with CBCT. Unlike medical CT, CBCT doesn't use standardized Hounsfield units, making density comparisons between patients—or even within the same patient over time—unreliable.
Radiation exposure varies dramatically between different CBCT devices and protocols. This underscores the importance of following the ALADAIP principle: keeping radiation As Low As Diagnostically Acceptable while being Indication-oriented and Patient-specific.
Advancements and Future Outlook in CBCT Technology
The field isn't standing still in addressing these limitations. Significant progress is being made in developing metal artifact reduction (MAR) algorithms that can clean up CBCT images affected by implants or restorations.
Integration represents the future of dental imaging technology. By combining CBCT data with information from intraoral scanners, clinicians can overcome limitations in both technologies. The scanner provides accurate tooth morphology while CBCT delivers the bone detail.
The future "virtual patient" is taking shape as developers work to integrate 3D facial scans with CBCT images. This comprehensive approach allows for more holistic treatment planning that considers both functional and aesthetic outcomes.
For these integrated approaches to reach their full potential, standardization of image formats (DICOM, STL, OBJ) is essential. This would allow seamless communication between different software platforms and devices.
Ultimately, the goal is simplification. By streamlining the digital workflow and reducing the number of steps involved, future CBCT applications will reduce potential errors while improving the patient experience through reduced chair time.
Your point of view caught my eye and was very interesting. Thanks. I have a question for you. https://accounts.binance.info/pt-PT/register-person?ref=KDN7HDOR
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me. https://accounts.binance.info/fr-AF/register?ref=JHQQKNKN
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me? https://www.binance.com/register?ref=IXBIAFVY